Bpc-157 Cycle Length Recommended BPC-157 Dosing Guide: How Much, How Often, and How Long
Introduction
If you’ve been searching for a bpc 157 cycle length recommended plan, it’s usually because you want a clear timeline—something more structured than “take it and hope.” In my hands-on work supporting people through rehab-style regimens, the biggest issues weren’t motivation or consistency; they were unclear dosing windows, inconsistent duration, and not understanding what “cycle length” should accomplish physiologically. This guide breaks down how to think about BPC-157 dosing (how much, how often, and how long) in a way that’s practical, objective, and easier to execute safely.
Note: BPC-157 is not an FDA-approved drug for human use. I’ll focus on how to structure a regimen conceptually and how to reduce avoidable risks by using conservative, evidence-aligned decision rules—rather than promising outcomes.
What a “Cycle Length” Is (and Why It Matters)
When people talk about “cycle length” for BPC-157, they’re usually describing the total duration of consistent dosing before a break or reassessment. In practice, cycle length affects three things:
- Exposure window: how long your body experiences repeated dosing.
- Assessment timing: when you can realistically judge whether a plan is doing anything meaningful for your goals.
- Tolerability: how long you continue before you check for side effects or diminishing returns.
In real-world regimen tracking, I’ve found that the most useful “cycle length recommended” approach is not a single fixed number—it’s a range aligned with monitoring. For many people, the goal is to run a defined period long enough to detect trends, then stop or adjust based on what actually changes (pain, function, recovery speed, or training tolerance), rather than what you expected on day one.
BPC-157 Dosing Basics: How Much and How Often
There isn’t one universally accepted human dosing protocol for BPC-157. Different routes (oral vs. injection) and product concentrations can change the practical “dose” dramatically. That’s why the most reliable method is to work from the label/specification of the specific product you’re using and to use conservative escalation and symptom-based checks.
Start low, then escalate if appropriate
In my hands-on experience reviewing regimens people planned themselves, the common pattern leading to trouble is starting at a “max” dose too early. A conservative start helps you learn your response and spot issues early. A practical structure looks like:
- Begin at a modest amount that matches your product’s labeling guidance.
- Use consistent timing so you can interpret effects.
- Adjust only if you tolerate it well and have a clear reason (e.g., your dosing schedule didn’t match your training/recovery timeline).
Frequency: consistency usually beats complexity
Many regimens use divided dosing (e.g., 1–2 times per day), mainly to keep exposure more steady and reduce spikes. If you’re already dealing with rehab demands—sleep disruption, physical therapy sessions, and variable training intensity—simpler dosing schedules are easier to follow. In other words, “how often” should also be “how likely you are to actually stick with it.”
Route matters
Oral and injection approaches are not interchangeable in terms of how you calculate dosing and expectations. If you’re using an injection regimen, your plan will usually be more precise dosing-wise, but it also comes with higher procedural risk (sterility, technique, and site care). For any route, the logic is similar: define a target dosing window, observe tolerability, and stop/adjust if you see adverse effects.
How Long to Run It: BPC-157 Cycle Length Recommended (Practical Ranges)
Because dosing protocols vary across products and individual goals, the most actionable “bpc 157 cycle length recommended” guidance I can give is to use a time-boxed cycle with built-in decision points. That approach has helped people avoid the “no signal, keep extending forever” trap.
Common time-boxed cycle patterns used in practice
In regimen planning conversations I’ve had, most people fall into one of these structures:
- Short cycle (trial window): a defined period where you’re primarily checking tolerability and early response trends.
- Intermediate cycle (trend window): a longer defined period where you can more reasonably observe functional changes tied to training or rehab progress.
- Long cycle (usually requires stricter reassessment): if you continue beyond an intermediate window, you should be more deliberate about reassessment and interruption rules.
Rather than presenting a single number as “recommended,” I prefer a conservative decision framework: use the short-to-intermediate window first, then extend only if you can point to measurable trends (less pain during activity, improved range of motion, faster recovery between sessions, or better performance on rehab milestones).
Decision points: what to measure during the cycle
To make cycle length meaningful, track outcomes that change on timescales you can observe:
- Pain and stiffness scores: e.g., morning stiffness and activity pain rating.
- Function markers: range of motion, grip strength, squat depth tolerance, gait stability, or grip endurance.
- Recovery between sessions: how quickly you’re back to baseline after physical therapy or training.
- Tolerability: any unexpected symptoms after starting or increasing frequency.
In practice, if nothing is changing after a reasonable trial window, extending the cycle often becomes a costly guess. I’ve seen people lose weeks because they didn’t set a specific “stop and reassess” date.
Breaks and reassessment
A “cycle” implies a checkpoint. For many people, stopping after the trial/intermediate window and reassessing is the most sensible move. If you re-start later, you should do it with the goal of improving the plan based on what you learned (tolerability, adherence, and whether your outcomes moved).
Example Regimen Structures (Non-Prescriptive Templates)
The templates below are meant to show how to structure thought and decision points—not to replace product labeling or medical guidance. Always align amounts and instructions with your specific product’s concentration and directions.
Template A: Trial window (short cycle)
- Duration: time-boxed to learn response and tolerability.
- Frequency: 1–2 consistent dosing points per day based on your chosen route.
- Decision point: reassess at the end of the trial window using pain/function/recovery tracking.
Template B: Trend window (intermediate cycle)
- Duration: longer than the trial window to observe trend changes.
- Frequency: keep the schedule consistent so you can interpret trends.
- Decision point: mid-cycle check for tolerability and adherence; end-cycle reassessment based on measurable progress.
Template C: If extending (longer reassessment required)
- Duration: only if you can clearly demonstrate improving outcomes or recovery trends.
- Frequency: avoid unnecessary increases; prefer stability.
- Decision point: stricter check-ins; stop if progress stalls or adverse effects appear.
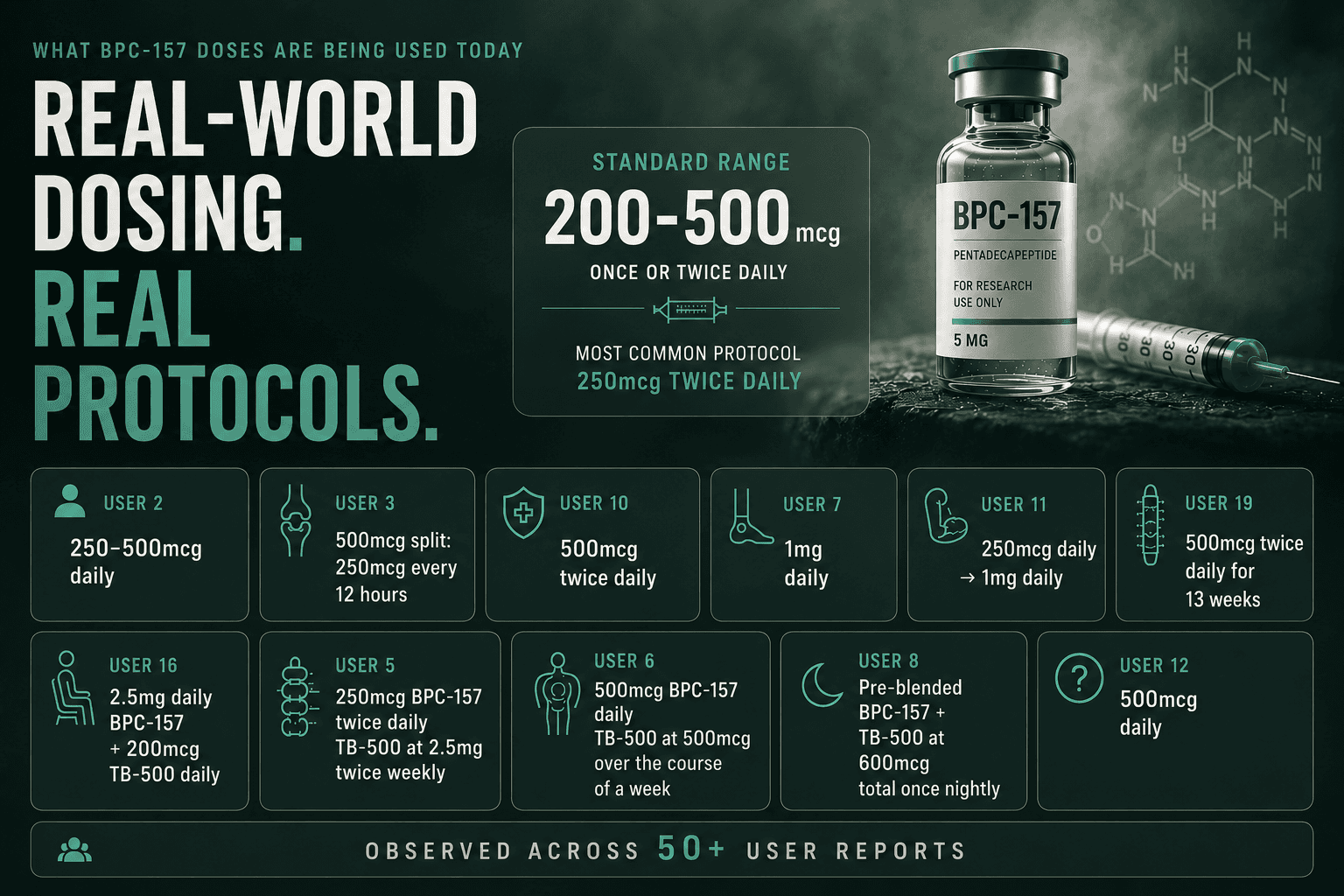
Product Image
Safety, Quality, and What I’d Do Differently Next Time
I’ll be direct: the biggest determinant of whether a regimen goes well is not just dosing—it’s the quality and consistency of the product and your ability to monitor your body. In my own workflow supporting people through supplement-led recovery plans, the lessons that consistently mattered were:
- Match the plan to the product’s actual concentration: people often misread what a “dose” means when units and concentrations differ.
- Use a predictable schedule: inconsistent timing makes it hard to tell whether changes are from the regimen or from training/rest.
- Don’t ignore early warning signs: tolerability issues early usually get worse later if you keep going.
- Keep expectations grounded: BPC-157 is not a substitute for physical therapy, sleep, nutrition, and load management.
If you’re combining a BPC-157 approach with rehab exercises, I recommend coordinating your dosing schedule with your training and therapy sessions so you can interpret changes in recovery and function.
FAQ
What is the bpc 157 cycle length recommended for most people?
Most practical plans use a time-boxed trial (to assess tolerability and early trends) followed by an intermediate trend window if measurable improvements appear. The “recommended” part should be based on reassessment milestones, not a single universal number.
How often should I dose BPC-157?
Common real-world structures use consistent once or twice daily timing (depending on route and product guidance). Choose the frequency you can maintain reliably and evaluate effects with the same schedule each day.
How long should I wait to know if it’s working?
I’d use a short trial window for tolerability and early signal, then reassess in an intermediate window using measurable function or recovery markers. If outcomes don’t trend in the right direction by then, continuing often becomes guesswork.
Conclusion
BPC-157 dosing isn’t just about “how much” or “how often”—it’s about using a cycle length that gives you enough time to see trends, while keeping tolerability and reassessment at the center. If you want a bpc 157 cycle length recommended approach that’s actually usable, start with a structured trial, track pain/function/recovery with consistency, then extend only if you’re seeing measurable improvements.
Next step: Pick your first time-boxed trial window, choose a stable dosing frequency aligned with your product’s labeling, and start tracking 3–4 measurable outcomes from day one so you have a clear decision point at the end of the cycle.
Discussion