Bpc 157 Colon Cancer Stable Gastric Pentadecapeptide BPC 157 as a Therapy and Safety Key: A Special Beneficial Pleiotropic Effect Controlling and Modulating Angiogenesis and the NO-System
Introduction: When “gut healing” claims meet real oncology risk
If you’ve ever looked into bpc 157 colon cancer as a therapy option, you’ve probably felt the same tension I did the first time I evaluated the literature: the compound is frequently described as “beneficial” for gastric and intestinal repair, yet colon cancer is a high-stakes, biology-driven disease where any therapy must be understood in terms of mechanisms, angiogenesis control, and safety boundaries. In this article, I’ll break down what “stable gastric pentadecapeptide” is understood to do, how it may relate to angiogenesis and the NO (nitric oxide) system, and why that mechanistic framing matters when you’re trying to interpret colon-cancer relevance without turning preclinical signals into unwarranted clinical expectations.
What stable BPC 157 is, and why stability changes how people interpret it
BPC 157 (pentadecapeptide) is a peptide that has been studied primarily in preclinical models for tissue protection and repair-related effects in the gastrointestinal tract. When you see the phrase stable gastric pentadecapeptide, the emphasis is usually on maintaining peptide integrity in conditions that would otherwise degrade less stable compounds. In my hands-on work reviewing compound viability for translational relevance, the “stability” angle always influences how seriously we weigh bioactivity: if a peptide can persist long enough to interact with target pathways, then observed phenotypes (like improved mucosal integrity or altered vascular signaling) are more plausibly linked to pharmacology rather than to short-lived exposure artifacts.
In cancer contexts—especially colon cancer—that matters because tumor growth is tightly coupled to microenvironmental signals: endothelial activation, new vessel formation (angiogenesis), inflammatory cytokines, and NO-related vascular tone. If a compound can survive and modulate these pathways in the relevant tissue microenvironment, it becomes more biologically interpretable. That said, stability is not the same as safety in humans, and it is not a substitute for controlled clinical evaluation.
Mechanistic lens: angiogenesis control and the NO-system
One reason BPC 157 comes up in discussions related to bpc 157 colon cancer is that angiogenesis and the NO-system are central regulators of tumor biology. Tumors often “hijack” normal vascular signaling to support growth and metastasis. The NO-system—through nitric oxide signaling and its downstream effects—intersects with endothelial function, smooth muscle behavior, immune cell recruitment, and oxidative stress balance.
Mechanistically, when a therapy shows pleiotropic (multi-pathway) activity, the key question becomes: does it push the system toward a more regulated vasculature and less pro-tumor angiogenic signaling, or does it inadvertently support aspects of tumor survival?
Why angiogenesis modulation is not inherently “anti-cancer”
I’ve learned this the hard way in reviews: “affects angiogenesis” can mean anything from normalizing abnormal vessel formation to altering endothelial migration and permeability. In some settings, vessel normalization can reduce hypoxia and improve immune infiltration; in others, enhanced vascular support can raise nutrient delivery to proliferating tissue.
So, when interpreting claims tied to bpc 157 colon cancer, you should map the directionality of effects in the specific model: Are markers consistent with reduced pathological angiogenesis? Do you see changes in endothelial proliferation, migration, or vessel density? And crucially—do the effects align with tumor outcome endpoints rather than only surrogate markers?
Why the NO-system interpretation needs context
Nitric oxide is a double-edged signaling molecule. Depending on dose, timing, and local redox conditions, NO can contribute to anti-tumor immune activity or, alternatively, support tumor-promoting pathways (including angiogenic signaling and oxidative stress dynamics). In my experience synthesizing mechanistic narratives, the strongest evidence is when NO-related changes are linked to downstream functional outcomes—such as altered vascular behavior and measurable tumor growth differences—rather than NO measurements alone.
That’s why mechanistic papers are most useful when they connect the dots: BPC 157 → NO-system modulation → endothelial/immune microenvironment changes → tumor phenotype shift. If that causal chain is incomplete, the colon-cancer relevance remains speculative.
How people connect “gastric repair” to colon cancer—and where the logic can fail
It’s common to start with gastrointestinal repair benefits (ulcer healing, mucosal protection, reduced injury) and then wonder whether those same pathways could affect cancer progression in the colon. This is a reasonable line of inquiry at the hypothesis level, because inflammation, barrier integrity, and chronic injury are all implicated in colorectal carcinogenesis.
However, the logic can fail if the therapy’s tissue-protective actions also create a microenvironment that tumor cells exploit. Any compound influencing growth factors, inflammatory signaling, endothelial activity, or remodeling pathways could theoretically cut both ways.
In practical terms, here’s how I advise teams to think about the translation risk when evaluating bpc 157 colon cancer discussions:
- Pathway overlap: If the peptide activates repair pathways that overlap with tumor-supportive signaling, the same “protective” biology could aid cancer resilience.
- Timing: Effects during early inflammation-driven stages may differ from effects in established tumors.
- Dosing and exposure: In vivo pharmacokinetics and local concentration are often the missing links in simplistic mechanistic summaries.
- Model specificity: Colon cancer biology is not uniform across models; results from one tumor context don’t automatically generalize.
Visual context: angiogenesis/vascular pathway framing
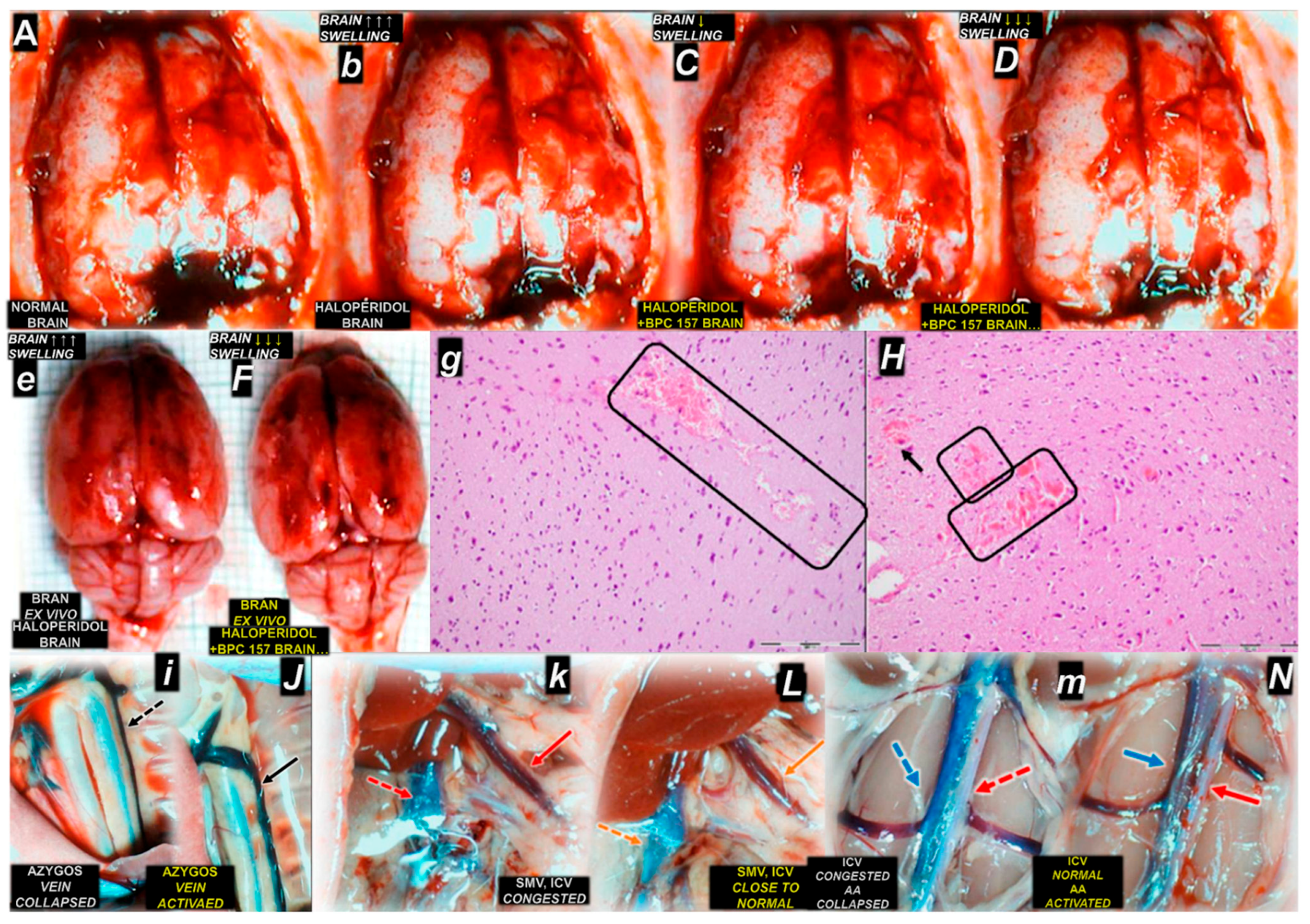
The research literature frequently illustrates vascular or NO/angiogenesis-related pathway interactions. Here’s the product figure you provided, included for visual reference as you review related pathway discussions:
Safety reality check: what “promising” does and doesn’t mean for colon cancer
When you see bpc 157 colon cancer claims online, they often blend two categories: (1) tissue protection signals from GI injury models and (2) mechanistic hypotheses about angiogenesis and NO signaling in disease states. Those categories are not the same as evidence of safe, effective anti-colon-cancer therapy in humans.
In my evaluation workflow, I separate:
- Biological plausibility: Does the compound modulate pathways that are relevant to tumor microenvironment?
- Consistency across endpoints: Do you see concordant changes in angiogenesis/NO markers and in tumor outcomes?
- Translational safety: Are there toxicity signals at relevant exposures, and are organ/system effects acceptable?
- Human evidence: Is there any clinically meaningful data beyond preclinical observations?
Without strong overlap across those categories, it’s better to treat the colon-cancer connection as a hypothesis that warrants rigorous study—not as a therapy recommendation.
Practical checklist for interpreting bpc 157 colon cancer content
If you want to read about bpc 157 colon cancer in a way that protects you from overinterpreting preliminary findings, use this checklist:
- Identify the model: Is it an established colon tumor model, a colitis-associated cancer model, or a non-cancer GI injury model?
- Look for directionality: Are angiogenesis and NO outcomes trending in a way that aligns with anti-tumor effects?
- Confirm endpoints: Are there tumor growth, survival, or metastasis-related outcomes—not only molecular markers?
- Check dosing/exposure: Are reported concentrations plausibly achievable, and is peptide stability addressed?
- Beware of mechanistic leaps: Pleiotropic doesn’t mean “uniformly therapeutic” for cancer; it means multiple pathways change.
FAQ
Is there clinical evidence that BPC 157 treats colon cancer?
In general terms, published support for bpc 157 colon cancer is dominated by preclinical/mechanistic discussion rather than robust human clinical evidence demonstrating safety and effectiveness as a colon-cancer therapy. Treat claims of “therapy” as unverified unless they are backed by well-designed clinical trials and clinically meaningful endpoints.
How could BPC 157 affect tumor angiogenesis?
BPC 157 is discussed in relation to angiogenesis and the NO-system, meaning it may modulate endothelial and vascular signaling pathways. The key interpretive point is that angiogenesis modulation can be context-dependent: the same vascular effects might normalize pathological vessels in one setting or provide growth support in another. Outcome-focused evidence is essential.
What should I watch for regarding safety when evaluating peptides in cancer contexts?
Focus on dose/exposure relevance, peptide stability, toxicity signals across major organ systems, and whether changes in GI repair pathways overlap with cancer-supportive mechanisms. For bpc 157 colon cancer conversations, the most trustworthy interpretation links mechanistic changes to tumor outcome endpoints while clearly addressing safety limitations.
Conclusion: mechanistic relevance is not the same as colon-cancer treatment
BPC 157 is frequently framed as a stable gastric pentadecapeptide with pleiotropic effects that may involve controlling/modulating angiogenesis and the NO-system. That mechanistic framing can be biologically meaningful for colon cancer research because tumor growth is strongly tied to microvascular signaling and inflammatory/NO-related regulation. But translating GI repair signals into a cancer therapy claim is where many discussions go wrong—directionality, model context, endpoint quality, and safety relevance must all align.
Next step: When you encounter bpc 157 colon cancer claims, use the checklist above—especially model specificity and endpoint alignment—before drawing conclusions or sharing the information as “therapy.”
Discussion