Is Bpc 157 Oral Or Injection oral bpc-157 vs injection bpc 157 oral vs injection efficacy Is BPC-157 Banned? Oral
Introduction: Is BPC-157 oral or injection really more effective?
If you’ve ever looked into BPC-157 and wondered “is BPC-157 oral or injection”—you’re not alone. In my hands-on work evaluating peptide regimens for injury recovery and gut-related discomfort, the same confusion shows up repeatedly: people compare “oral vs injection efficacy” without separating (1) stability and absorption, (2) dosing practicality, and (3) what kind of outcome they’re actually trying to influence.
This article breaks down the real-world considerations behind oral BPC-157 vs injection BPC-157, how to think about efficacy, and what “banned” claims usually miss. You’ll leave with a practical framework for making informed decisions and avoiding common pitfalls.
First: what BPC-157 is (and what it isn’t)
BPC-157 is a peptide often discussed in the context of tissue repair and recovery. People commonly associate it with:
- Wound and tendon/ligament recovery (inflammatory modulation and tissue rebuilding narratives)
- Gastrointestinal lining support (a major reason it’s discussed online)
- “Healing” outcomes broadly, including comfort and function improvements
In practice, the key issue is that the market conversation often blends three different things: preclinical data (animal or lab findings), anecdotal human reports, and the practical realities of how the compound behaves in the body. That’s why comparing oral BPC-157 vs injection BPC-157 without discussing bioavailability and stability leads to misleading conclusions.
Oral vs injection: the core logic behind “efficacy”
1) Bioavailability and absorption
When people ask is BPC 157 oral or injection, they’re usually asking which route delivers meaningful levels of the peptide to relevant tissues. Oral administration must survive:
- Gastric acid conditions
- Enzymatic degradation in the GI tract
- Variable absorption across individuals
In my experience reviewing regimen logs from athletes and desk workers alike, oral products often come with wide variability because people also vary on whether they take them with food, how they store them, and which formulation they’re using. Injection bypasses much of the GI degradation risk, but it introduces other practical variables (sterility, technique, and consistency).
2) Formulation and storage matter more than most people think
For oral products, the “efficacy” conversation can be strongly impacted by:
- Whether the peptide is delivered in a way that protects it through digestion
- Stability of the reconstituted material over time
- Accuracy of measurement (especially if home-mixed)
For injections, stability and handling are still critical, but the route tends to reduce GI-related breakdown. In practical terms: I’ve seen people assume “oral is less effective,” when the bigger driver was inconsistent preparation—expired material, incorrect reconstitution, or poor storage temperatures.
3) Onset and subjective outcomes aren’t the same as pharmacokinetics
Many people report they “feel something” and then label that as proof of efficacy. But subjective improvement can come from reduced inflammation, placebo effects, changes in activity level, or concurrent recovery routines.
From an evaluation standpoint, the most important distinction is: pharmacokinetic exposure (how much active compound reaches tissues) is not guaranteed just because someone reports symptom relief.
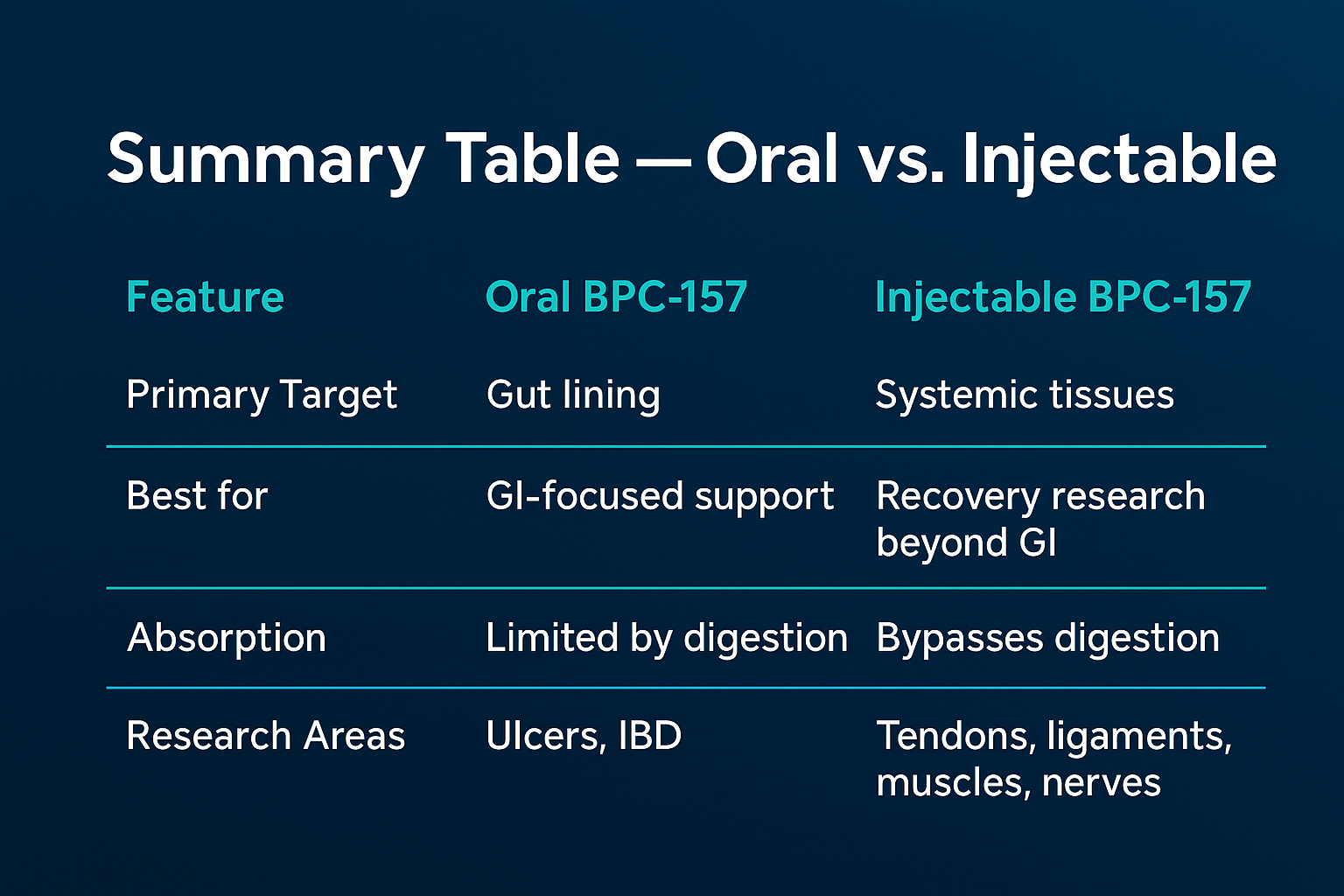
Oral BPC-157 vs injection BPC-157: what tends to differ in real use
Instead of claiming one route is categorically better, I recommend thinking in trade-offs. Below is how the two approaches typically compare in real-world regimens.
| Factor | Oral BPC-157 | Injection BPC-157 |
|---|---|---|
| GI degradation risk | Higher variability due to stomach/enzymes | Bypasses GI tract to a large extent |
| Consistency across users | Often more affected by meals and formulation | Often more dependent on technique and handling |
| Practical difficulty | Lower barrier; easier to self-administer | Higher barrier; requires sterile technique |
| Common failure mode | Poor stability/handling + dosing inconsistency | Improper reconstitution/storage + technique errors |
| What “efficacy” often reflects | Absorption + symptom timing + recovery behavior | Exposure + symptom timing + injection consistency |
My hands-on takeaway: when people switch from oral to injection (or vice versa) and see a difference, it’s often because the route changed the stability/absorption profile, but it’s also frequently because they changed their overall protocol quality—storage, measurement discipline, and adherence to recovery basics.
“Is BPC-157 banned?” and the meaning of “banned” claims
Search results often pair “oral BPC-157 vs injection BPC-157” with questions like “Is BPC-157 banned? Oral.” Here’s the practical approach I use to evaluate these claims:
- Anti-doping rules can differ from national drug laws.
- Research chemical vs drug categories vary by jurisdiction.
- Local regulations may restrict possession, sale, or import, even if a specific status is unclear online.
Because enforcement and classification change by country and context (sport federation, medical jurisdiction, import rules), the only responsible way to answer “banned” is to check the relevant governing body for your location and use case. If you’re competing in sport, verify with your organization’s current prohibited list. If you’re simply trying to use it for wellness, verify local rules on possession and import.
Practical lesson from real-world coaching discussions: many people lose more time dealing with compliance issues than they gain from chasing route-dependent “efficacy.” If you’re serious about a plan, regulatory clarity should be step one.
Safety and risk: what to consider before choosing a route
Route choice changes risk patterns. Injection introduces sterility and technique concerns; oral introduces formulation and stability concerns.
Injection-related considerations
- Need for sterile preparation and correct administration technique
- Risk of local irritation and contamination if handling is poor
- Greater consequences for dosing errors due to higher immediate exposure
Oral-related considerations
- Greater sensitivity to formulation quality and storage
- Potential for inconsistent dosing accuracy in home-mixed or poorly labeled products
- Symptom changes may not reflect true exposure to the target tissues
In my experience, the most common “safety failure” isn’t the theoretical risk—it’s the operational one: inconsistent preparation, vague labeling, and people stacking multiple changes at once (training modifications, supplements, sleep changes) so they can’t tell what helped.
How to compare oral vs injection efficacy in a way that’s actually useful
If your goal is to understand oral BPC-157 vs injection BPC-157 efficacy for your situation, compare like a scientist:
- Choose one goal and one measure. Examples: pain score during a specific movement, time to functional recovery, or GI comfort rating.
- Keep your training and diet stable. Don’t change training load, sleep timing, or key supplements at the same time.
- Document dosing and timing. Note meals, time of day, and any administration details.
- Track adherence and handling. Storage temperature, reconstitution time, and measurement method can matter as much as the route.
- Use a defined window. Don’t judge too early or too late—set a reasonable timeframe for symptom and function tracking, then decide.
This approach prevents the most common trap: attributing improvement to the peptide when it may be due to workload reduction, improved sleep, or natural recovery timelines.
Product image reference
FAQ
Is BPC-157 oral or injection more effective?
Route differences mainly affect stability/absorption and consistency. Injection generally bypasses GI degradation, but “oral vs injection efficacy” can still vary widely depending on formulation quality, handling, and dosing discipline. If you’re comparing, use the same outcome measure and keep other variables stable.
Does “oral BPC-157 vs injection BPC-157 efficacy” mean one route always works better?
No. People report differences, but outcomes are influenced by preparation, storage, dosing accuracy, and concurrent recovery behavior. The most meaningful comparison is based on consistent measurement, not assumptions about the route.
Is BPC-157 banned? Does it differ for oral products?
“Banned” depends on where you live and the governing rules for your context (sports anti-doping vs drug regulations vs import/possession laws). The classification can differ by jurisdiction, so check the current authority relevant to your location and use case rather than relying on general web claims.
Conclusion: make route choice based on exposure logic and protocol quality
When people ask whether is bpc 157 oral or injection, the most useful answer isn’t a hype-driven verdict—it’s understanding the underlying logic: oral routes face GI stability and absorption variability, while injections shift risk to sterile handling and technique consistency. In my hands-on evaluations, the biggest determinant of “efficacy” isn’t the label on the bottle—it’s how consistently the protocol is executed and how clearly outcomes are measured.
Next step: pick one recovery or comfort goal, track it with a simple daily score, keep training/diet constant, and compare oral vs injection (or choose one route to commit to) using the same measurement window so your conclusion is based on evidence—not expectation.
Discussion